Where There is Despair, Let Me Bring Hope: Assisted Suicide, the Moral Dissociation Curve and Compassionate Love
I suspect several of those reading this essay have had patients like the one described. How are we to care for this suffering person? Do we acquiesce to his request if we’re in a state where assisted suicide is legal? As a medical culture and a society, we are at a crossroads as to how we will care for the aging and infirm populations of our graying nation.

Richard W. Sams, II, MD, MA
by Richard W. Sams, II, MD, MA
“The knowledge of good and evil seems to be the aim of all ethical reflection. The first task of Christian ethics is to invalidate this knowledge.”
Illustrative Case
You admit a 76-year-old debilitated male to a long-term care facility with a history of coronary disease, advanced kidney disease, heart failure, peripheral neuropathy and failure to thrive. He has severe neuropathic pain in his lower extremities, unbearable pruritis and constant nausea. He has seen multiple specialists who have attempted unsuccessfully to improve his symptoms. He is despairing and depressed. He expresses he can no longer live like this and repeatedly requests you give him something to end his life.
The Normalizing of Assisted Suicide
I suspect several of those reading this essay have had patients like the one described. How are we to care for this suffering person? Do we acquiesce to his request if we’re in a state where assisted suicide is legal? As a medical culture and a society, we are at a crossroads as to how we will care for the aging and infirm populations of our graying nation. Assisted suicide was considered morally illicit for millennia as proscribed in the Hippocratic Oath. This has changed with the rise of a materialist ethic based on philosophical naturalism, which rejects the idea there are any supernatural realities, including universal moral laws. Assisted suicide is now permissible in 10 states—California, Colorado, Hawaii, Montana, Maine, New Jersey, New Mexico, Oregon, Vermont and Washington—and the District of Columbia. Ballot initiatives and legislative proposals are ongoing in several other states to legalize assisted suicide. Some proponents are calling for expansion of the practice, to include those with chronic non-terminal conditions, mental health conditions and those simply “tired of life.” Some advocates declare there should be no criteria. If a person desires to die, the physician should provide the service. Others say we should practice euthanasia like Canada, the Netherlands and Belgium, personally administering a lethal cocktail of medicines to the suffering who desire death.
Proponents and advocacy groups are flooding our state legislatures, medical journals and web spaces with euphemisms to normalize this sea of change in healthcare. The primary U.S. national advocacy group, once called the Hemlock Society, is now Compassion & Choices. What was originally mercy killing, then assisted suicide and euthanasia are now called “Medical Aid in Dying,” “MAID” and “Death with Dignity.” All these euphemisms eclipse the reality the physician—and in some locales a physician assistant or nurse practitioner—is personally acting to help terminate a patient’s life.
The euphemism “aid in dying” blurs the distinction between assisting someone to die well naturally and assisting them by taking their lives prior to a natural death. Dying is an inexorable journey of indeterminate length not yet completed; death is the terminus ad quem, the final destination, the irreversible cessation of life. Palliation of the former is the goal of compassionate care; the latter is the goal of assisted suicide, euthanasia and “MAID.” Helping someone to die a natural death well implies addressing all aspects of pain and suffering, maximizing quality of life despite the limiting conditions and addressing emotional and spiritual problems. Assisted suicide and euthanasia require none of the above to take place. They only require a person having a period of suffering to ask someone to assist them to end their lives. Both are attempting to help a suffering person. Only one is terminating the life of the suffering patient. These realities are not expressed by proponents, only that we are helping patients fulfill their wishes about their own lives.
The Lie of Autonomy is the Driving Force
CMDA’s state advocacy and ethics arm, the American Academy of Medical Ethics (AAME, ethicalhealthcare.org), is working to prevent the spread of assisted suicide laws across the country through advocacy within the state medical societies, specialty societies and engaging with state and federal government officials. Even as the AAME is working, an endless supply of funds and proponents are actively pushing for the normalization of the practice. CMDA Senior Vice President of Public Policy and Bioethics and AAME President Dr. Jeffrey Barrows recently stated that turning the tide of this trend is incredibly difficult politically since political discourse and legislation are downstream from culture. Cultural trends guide policy, laws and practices.
What is the fundamental ethos in our society resulting in the acceptance of assisted suicide and euthanasia by such large numbers of people? In a word, autonomy. All proponents of these practices cite autonomy of the person as the primary justification. The popular understanding of autonomy is, you are your own self-legislator: auto – self, nomos – law. You decide what is right for you. The notion of autonomy is the founding concept of democratic liberalism and medical ethics. On a deeper level, this idea reflects we have rejected God in being our Lawgiver, our Reference Standard and our Compass. The closing stanza of the poem Invictus by Henley reflects this reality: “It matters not how strait the gate, how charged with punishments the scroll, I am the master of my fate: I am the captain of my soul.”[2] A common refrain from some is, “I can choose to die on my own terms.”
Where has philosophical naturalism, the notion autonomy and the subsequent nihilism left us as a culture? We have epidemics of depression, anxiety, drug use and deaths of despair with more than 150,000 persons dying from drug overdosages or suicide per year.[3] Even before the COVID-19 pandemic, the U.S. life expectancy decreased secondary to suicide and drug overdosages.[4] Amidst our despairing culture, we are now asking physicians to assist our suffering patients to end their lives.
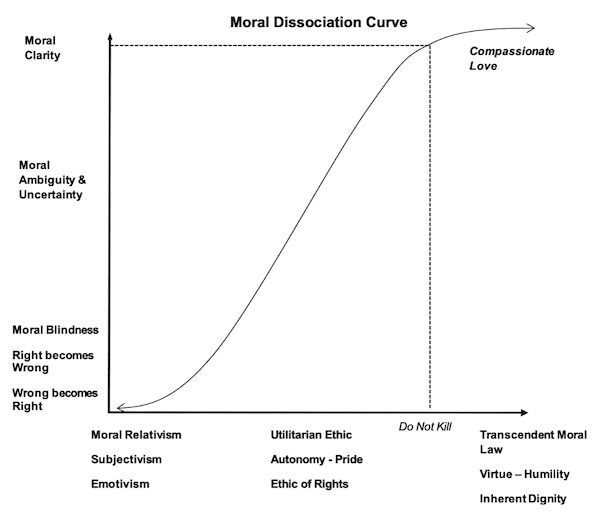
The moral dissociation curve helps us understand how leaders in our own profession have come to the point of justifying physicians ending the lives of their patients. See Figure 1 for reference. The moral dissociation curve serves as a bridge between meta-ethical theory, applied ethics and their relationship to moral clarity on a given issue. It reflects an a priori commitment to the presence of transcendent moral law to include universal moral laws and virtues. C.S. Lewis provided the best-known defense of transcendent moral law in his book The Abolition of Man. He calls transcendent moral law the Tao (the way), and he demonstrates that consistent fundamental moral values, virtues and laws have been present in independent civilizations throughout human history. When we reject the fundamental moral law, do not kill, and the corollary moral principle for healthcare professionals, do not intentionally end the lives of your patients, and are guided only by autonomy and a utilitarian ethic, our moral vision dims. If, as a culture, we completely reject universal moral law or any of its corollary principles and descend into nihilism, we are left with right and wrong determined by the loudest voice, the majority vote or the strongest arm. What is right or good becomes purely subjective, guided only by emotion and impulse. This is the situation in our cultural moment. Pitirim Sorokin called it a sensate culture; one dominated by materialism and hedonism.[5]
A Better Way
As Christ followers, we intuitively understand the reality of transcendent moral law—moral laws and virtues in existence from eternity. We humans did not devise them, nor did the state. We discover them with the eyes of our heart when we humbly recognize we are not our own and are accountable to One bigger than ourselves. We know God is the Reference Standard.
We also recognize we are not autonomous. In the words of the poet Jon Donn, “No man is an island, entire of itself. Every man is a piece of the continent, a part of the main…any man’s death diminishes me.”[7] As Wendell Berry declared in The Unsettling of America: Culture and Agriculture, autonomy is an illusory condition, “suggesting that the self can be self-determining and independent without regard for any determining circumstance or any of the obvious dependences. This seems little more than a jargon term for indifference to the opinions and feelings of other people. There is, in practice, no such thing as autonomy. Practically, there is only a distinction between responsible and irresponsible dependence.”[8] Humans are not autonomous islands floating in the sea of humanity. We are highly interdependent upon each other. What affects one directly, affects all indirectly.
Finally, we recognize ethics is God’s mother tongue, His eternal word. Without God, ethics is nothing, it’s gibberish. The eternal commands, such as do not kill, serve as guardrails from our base temptations as humans. We know our suffering patients do not need physicians willing to take their lives. They don’t simply need physicians who say no to assisted suicide. They need virtuous physicians, nurses and others in healthcare who are willing to walk alongside them in their suffering—the true meaning of compassion. If unable to cure, we seek to relieve symptoms and care for the dying to the point of natural death. The virtues of medical care—presence, empathy, fidelity to the person, courage, wisdom, temperance, humility and bedside grace—should guide and shape our actions to our suffering patients. These are tied together by agape love, which seeks the highest good for the patient. Social science researchers call this type of love compassionate love. As Christian healthcare professionals, compassionate love needs to be our hallmark when caring for the suffering—and when we engage in advocacy and policy formation.
Response to Illustrative Case
You listen carefully to your hurting patient, striving to understand the reason behind his request. You sense he feels powerless in the face of his decline and incapacitating symptoms. You express to him that you are going to work with him to get the symptoms under control and, with the help of your multidisciplinary team, help him achieve the best life possible. Given the palliative nature of his condition, you offer to schedule him with lower dose opioids to first relieve the pain. He is grateful. He takes the medicine only for a matter of days, his pain is improved and he states he doesn’t need it anymore. You perform a careful medicine reconciliation and recognize the myriads of medicines provided by the specialists produce side effects that include his symptoms. You de-prescribe judiciously and provide a counter-irritant cream for his neuropathy and schedule antinausea therapy, and medicine for his depressive symptoms. All his symptoms abate, and he ceases to ask to have his life ended. You visit him regularly to get to know him as a person, expressing interest and care for him and his family. Each time you see him, he expresses gratitude for how you have taken care of him.
Concluding Reflection
We are at a critical time as a culture. It needs not consequential arguments against assisted suicide. It needs a resuscitation of God consciousness. An ethics founded in transcendent moral law can serve as a gateway to God. We can no longer shirk back from basing our arguments on eternal laws. We do need to be non-sectarian in nature. We simply call for a humble recognition that there are moral laws we did not devise as humans but are to follow. In so doing, we may mend the conscience of our blinded culture and ascend the moral dissociation curve. As Bonhoeffer declared, the fruitless reflections of secular ethics need to be invalidated. We need to courageously declare that we must stand firm in the Hippocratic Ethic in protecting the vulnerable through all stages of life, seeking the ultimate good for the patient with compassion and moral integrity, and say “no” to willfully ending our patients’ lives.
Even more important, our despairing culture and our patients need an infusion of hope, not lethal substances. As Anne Frank declared in her diary, “Where there is hope, there is life. It fills us with courage and makes us strong again.”[9] As Christians, we know the Good News for the despairing patient and the source of hope and faithful love. In our fight against the cancer of assisted suicide, let us not be afraid to hold out the banner of our hope to our suffering patients and our policymakers. We may or may not stem the tide of assisted suicide laws, but we will be a beacon of light to the suffering.
Acknowledgements
Dr. Sams would like to thank his friend Dr. Pete Jaggard for collaborating as a co-author in other publications on the topic. A number of his ideas previously expressed in those papers are present in this article.
Get Involved
As one of the core aspects of CMDA’s ministry efforts, CMDA’s Advocacy team is dedicated to serving as a Christian healthcare voice in the public, to the media and to the government. And we do that through our grassroots advocacy efforts on both state and federal levels as we stand together to protect the vulnerable and bring the hope and healing of Christ to the world through advocacy. For more information and to get involved, visit cmda.org/advocacy.
About the Author
Richard W. Sams, II, MD, MA, is a graduate of Boston University School of Medicine and Waukesha Family Practice Residency. He completed an master of arts in bioethics at Trinity International University and the faculty development fellowship at Madigan Army Medical Center. He completed a 22-year career in the U.S. Navy. He is a Professor in the Department of Family and Community Medicine at the Medical College of Georgia and Medical Director of Georgia War Veterans Nursing Home, where he teaches, practices and conducts research. He has 36 peer-reviewed publications and is a founding board member of the American College of Family Medicine. He is currently the CMDA Georgia State Representative and one of the state directors for the AAME. Dr. Sams and his wife Teri have been married for 35 years, and they have five children and three grandchildren.
[1] Bonhoeffer, Dietrich. Ethics. New York, Macmillan Publishing Co, 1965.
[2] https://poets.org/poem/invictus
[3] https://www.cdc.gov/suicide/facts/data.html#cdc_data_surveillance_section_3-suicide-deaths-plans-and-attempts-in-the-united-states
[4] https://pmc.ncbi.nlm.nih.gov/articles/PMC8579049/
[5] Johnston, B. V. (1998). PITIRIM A. SOROKIN AND SOCIOLOGICAL THEORY FOR THE TWENTY-FIRST CENTURY. Michigan Sociological Review, 12, 1–23. http://www.jstor.org/stable/40969020
[6] Sams II, R. W. (2024). The Moral Dissociation Curve, Blind Spots and Prescribing Death in Canada. Canadian Journal of Bioethics / Revue canadienne de bioéthique, 7(4), 125–130. https://doi.org/10.7202/1114969ar
[7] https://allpoetry.com/No-man-is-an-island
[8] Berry, Wendell. The Unsettling of America: Culture & Agriculture. San Francisco, Sierra Club Books, 1977.
[9] Frank, Anne, 1929-1945 author. The Diary of a Young Girl: the Definitive Edition. New York: Doubleday, 1995.