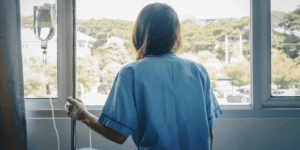
Street Medicine: Running a Free Clinic in the Era of COVID
When I contracted COVID-19 on March 18, 2020, it was so early in the outbreak of the pandemic that my illness sent shock waves of fear through Inland Vineyard Medical Mission and Free Clinic where I serve as director. Everyone on our team was worried, including our student workers. How would we keep our team safe? And how would we still treat our patients? For most of our patients, we are their main source for both food and medical care. Where would they go if we suddenly shut our doors?
When I contracted COVID-19 on March 18, 2020, it was so early in the outbreak of the pandemic that my illness sent shock waves of fear through Inland Vineyard Medical Mission and Free Clinic where I serve as director. Everyone on our team was worried, including our student workers. How would we keep our team safe? And how would we still treat our patients? For most of our patients, we are their main source for both food and medical care. Where would they go if we suddenly shut our doors?
Almost immediately, we knew we couldn’t continue practicing “street medicine” the same way we had been before COVID arrived at our doors.
What were we going to do?
Street Medicine Before COVID
Inland Vineyard Medical Mission and Free Clinic is in Riverside County, California, which is also called the Inland Empire, a sprawling collection of cities 50 miles east of Los Angeles. As a team, we provide primary care services and food assistance services to underserved, low-income patients. With a focus on serving the underserved in their local neighborhood and community, volunteer healthcare professionals and students in training take vital signs and provide basic procedures or offer resources for further care.
Because of the work we do, our team is an incredibly close-knit group. As the director of the clinic, I do my best to foster a spirit of unity and teamwork. We usually pray before and after events, and some of the volunteers who are from various backgrounds, religions and cultures are always respectful during this time. Much of our team consists of undergraduate pre-health professional students, physician assistant students from the University of La Verne and medical students from University of California, Riverside (UCR), School of Medicine. The undergraduate students all rotate leadership roles every three months, which consists of inventory, administration, equipment maintenance, making sure each outreach event has stocked bags ready to go, working with the church pantry to get food donations out to the streets, training other new students to take vital signs, scribe, maintain our electronic medical records and more.
Zahid Mustafa, a graduate from UCR, is the first of any of our volunteers to secure a grant, which helped expand the church pantry and obtain iPads for scribing while we expanded our telemedicine services. He also helped develop more patient education materials and secured a generator when we would work into the darkness helping the migrant farm workers who needed medical attention after laboring hard in the fields in East Coachella Valley.
Street Medicine During COVID
In early March 2020, COVID-19 had just been recently reported in the state of Washington, plus some cases in northern California. It had not been widely reported throughout the United States at the time, but I knew it was likely circulating in southern California already. Masks had not yet been mandated, nor were there any social distancing protocols implemented yet.
We had been going through our normal routines when my symptoms started on March 18, 2020, with the aches and pains associated with a fever, plus a loss of taste and smell. The loss of taste and smell was not yet a widely reported symptom of the virus, but I knew this was a unique symptom beyond any other viruses I had studied. It turns out I had contracted the infectious virus while at a Kaiser Hospital in Los Angeles for 12 hours while waiting for my grandmother’s heart surgery two days prior.
After communicating with the public health department in my area, I was finally able to schedule a test after informing them that I was scheduled to see patients in the next few days. When my husband started developing symptoms too, I was also able to get him scheduled for a test since he is a public school teacher and was supposed to be at the elementary school handing out lunches and homework, as all California schools had closed just five days prior.
Everything came crashing down with the call from a public health doctor when my test results arrived. I was positive for COVID-19. By then, my mild symptoms had quickly turned into crushing fatigue, horrible myalgias making it difficult to move, bone-breaking chills and violent coughing causing my ribs to be sore while alternating and max dosing on ibuprofen and acetaminophen. When battling with a 104-degree temperature with a pre-existing heart condition, my heart began to re-flare: pre-ventricular contractions and severe palpitations. At that point I faced my own mortality and thought, “If there is any time that I am going to die from this virus, tonight is the night,” especially as my breathing became more difficult. It seemed there was no way out of the darkness closing in.
However, I simply could not accept death without a fight, as I have young children who needed a mother. Having lost our own mother to breast cancer at a young age, my sisters and I know the tremendous toll that type of loss can take on young children.
“Is Mommy going to die tonight?”
In the midst of my own suffering, these haunting, whispered words of one of my daughters to my husband made me realize what surrendering to COVID-19 truly meant. I placed a defibrillator near me on the bed, purchased years prior due to an existing heart condition. I hoped my husband or oldest daughter could operate it properly by following the prompts if I had a sudden cardiac arrest, yet it brought little comfort as it could not shield me from the onslaught of terrifying thoughts in my delirious state.
While I was at home battling the virus and my fear, Zahid and the other student leaders at the clinic were also facing their fears about COVID, now that it had hit so close to home. One of our student volunteers expressed that hearing about my infection “was the point at which it felt like the walls [of COVID-19] were starting to close in.” It “struck like a bolt of lightning,” and he “was scared about getting COVID-19 as well and potentially spreading it to other people, particularly his parents and grandmother that he lived with.”
Everyone on the team was worried. Over the course of multiple virtual conversations, an important insight began to crystalize:
If we were fearful, the vulnerable members of the
community we serve must be even more so.
Our team at the clinic needed to display the same determination and fortitude I was showing in my resolve to beat the virus. One of our student volunteers asserted that we needed to be models for the community because, “If we cannot control our fear and respond appropriately, how can we ever expect our patients to?”
As a clinic, it was scary to cease operations and leave at-risk patients without care. But how could we continue to serve those who rely on us without contributing to the further spread of the virus? With COVID-19 cases rising, telemedicine seemed like a logical solution. However, as we reflected on the situation, we realized that not all of our underserved patients have access to high-speed internet. Furthermore, many of our patients also depend on us for their nutritional needs. We still needed a way for our patients to pick up food for themselves and their families from our clinic.
After more thinking and conversation, the team decided to convert the clinic to a drive-thru model. Our drive-thru free clinic uses telemedicine to supplement our services, allowing for both in-person and virtual visits. We run the drive-thru free clinic in the parking lot of the church building we previously worked out of, which was forced to close at the onset of the pandemic due to statewide lockdown orders in California. Having the clinic in the same location makes it easy for former patients and members of the community to find us. Bright orange traffic cones replaced hallways to indicate where patients are to go. When patients first enter the drive-thru, they are able to pick up boxes of food for themselves and their families. At the next stop in the drive-thru, patients can get medical care. The drive-thru model allows patients to remain in their cars throughout their stay at the clinic, reducing the risk that they may infect others. Holding the clinic outdoors also reduces the risk that an infected patient will transmit the virus, while we also wear extra protection such as face masks, shields and gloves. Alternatively, patients can virtually schedule a telemedicine appointment through Zoom and receive medical care from the comfort of their own homes. All of these modifications have brought us tremendous joy since they allowed us to continue providing care to vulnerable members of our community during the pandemic.
Many of the patients we have seen since the pandemic started are still very worried. We have noticed that fear manifests most strongly in those who think they will lose a loved one to the virus. One of the most memorable interactions we have had was with a frantic man who believed his wife would die when she contracted COVID-19. Providing him information about the disease in a manner he could understand provided reassurance. Also useful were the personal insights his care team offered based on my experience as someone who had been infected with COVID-19. Everyone involved agreed it was quite rewarding to help calm the patient, and we continue to check in on this patient, whose wife is doing well.
Implementing the drive-thru model has been a success, giving both our staff and our patients comfort while dealing with the fear caused by the pandemic.
For all of us-both patients and healthcare professionals-COVID-19 was a learning experience. For our clinic, there’s no question we were all learning together as we faced our fears, faced what seemed to be a losing situation and faced the virus head on with resilience and determination.
A year later, we loved being able to move back into the church building-but with some changes. We now have chairs outside for patients who prefer to visit us outside due to concerns about the virus, plus we continue to offer the drive-thru and telemedicine models for patients who like to utilize those options as we still battle the ongoing pandemic.
This experience showed us that we cannot wait for perfect circumstances to care for the vulnerable. Street medicine is an absolutely crucial part of helping the underserved in our community, and we weren’t going to let the virus stop us from serving our community. And because of that, we had to be willing to adapt, to create new processes and methods, so that we can continue to treat the patients in front of us.
If you’re waiting for the perfect circumstances to present themselves before getting involved in caring for the vulnerable in your local community, don’t wait any longer. COVID-19 has proven that we are part of the human tapestry, and it’s shown us more than ever that we have a responsibility to care for and nurture each other in this incredibly stressful time. It is normal to be afraid, but what really counts is how we respond to it. We should not let the weight of fear deter us from doing the right thing.
Learn More
Are you interested in learning more about how you can serve the underserved in your local community? Join us at Remedy 2022, a healthcare missions conference designed to help you listen for and follow God’s call on your life to serve and practice right here in your own backyard in the U.S. For more information, visit www.cmda.org/remedy.
About the Authors
Jennifer Zamora, DHSc, MPAP, PA-C, is Professor of Practice and Director of Didactic Education University of La Verne, Master of Science, Physician Assistant Practice Program, where she is restructuring and modifying the current curriculum, assessment and appeal to ARC-PA regarding accreditation standards, interviewing all guest lecturers and mentoring and training new faculty. She personally teaches the pediatric and infectious disease series and assist in clinical skills. She also designed and executes the live model and standardized patient program, OSCE exams, simulations and hands-on workshops. She is working to incorporate inter-professional education (IPE) and inter-professional practice with the PA students. She was a founding faculty member of California Baptist University (CBU MSPAS) PA Program and guest lecturer at University of Southern California (USC), Keck School of Medicine. She was also a founding faculty member with a team from six other schools and disciplines for SoCal HEAL IPE (https://socalheal.org/) and serves as the co-director and clinical faculty at UCR School of Medicine (UCR SOM). As a previous clinical preceptor, she trained numerous physician assistant, nurse practitioner and medical students in the field from various programs including USC, Western University, Azusa Pacific, University of Kentucky, University of Maine and UCR SOM. Currently, the family medicine clinic and street medicine outreaches is a place where UCR MD students rotate at as well as ULV PA students, and she teaches during live patient encounters while at the clinic. Jennifer would like to thank all the volunteers who have helped keep the free clinic running during the pandemic, especially Zahid who helped with this piece and the grant they recently received to serve the underserved. Most importantly, Jennifer is honored to be a mother of two daughters and a wife of 20 years to her husband. God is good!
Zahid Mustafa, BS, is a Magna Cum Laude graduate in biology from UC Riverside. After graduating from UC Riverside, he started volunteering at Vineyard Free Clinic, where he is currently on the leadership team as a clinic coordinator. When the pandemic started, he helped launch a drive-thru model of the free clinic, which was featured in U.S. News & World Report. He also helps write grants for the clinic. Grants he has obtained from the National Association of Free and Charitable Clinics, CPPS Heritage Mission Fund and Google have kept the clinic’s medical and food distribution programs running through the pandemic. He is also a reviewer for the Journal of Student-Run Clinics. Outside of his work with free clinics, Zahid works as a medical researcher, where he has published nine peer-reviewed articles, including one in the Proceedings of the National Academy of Sciences.