A Time to EMBRACE Recovery
As those called to the healing profession, we have all lived and practiced through old and unprecedented new challenges in our careers. We can all agree the last few years have surely been unlike any we have ever experienced before in our lives.

Darren Caparaso, MD
by Darren Caparaso, MD
“Ever since I included God into my recovery, I’ve actually found RECOVERY. Studying His Word and implementing it into my life gives me LIFE.
Jesus really does save!”
—Robin
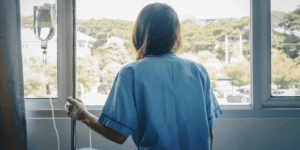
As those called to the healing profession, we have all lived and practiced through old and unprecedented new challenges in our careers. We can all agree the last few years have surely been unlike any we have ever experienced before in our lives. Frontline healthcare workers felt the brunt of a pandemic on a daily basis, while also enduring the devastating impact of yet another challenge of a public health crisis that continues to escalate.
That crisis is addiction.
For the first time in our nation’s history, fentanyl overdoses/poisonings have surged to become the number one cause of death for ages 18 to 45, according to the U.S. Centers for Disease Control and Prevention. It’s a shocking and alarming statistic. Our nation experienced approximately 107,600 overdose deaths in 2021 alone—soaring to become the highest ever recorded.
As a family medicine physician for nearly 30 years, it is an honor and privilege to be involved in patients’ lives, as the patients I treat become family to me. It is a true joy celebrating all the milestones in the lives of these patients, including newborn babies, weddings, athletic awards, academic accomplishments and vocational achievements. Of course, the journey also includes entering the sufferings of people and family members during the darkest times of those experiencing addiction and its terrible aftermath of broken bodies, broken souls, broken spirits, broken relationships and even the shock of sudden death. As the Bible says in Romans 12:15, I strive to “Rejoice with those who rejoice; mourn with those who mourn.”
My patients, my community and my church feel the pain and heartbreak of the growing addiction health crisis. More than likely, you see the same pain and heartbreak in your practice and in your city. However, despite the suffering, we have HOPE!
I am grateful to have grown up and continue to live in Buffalo, New York, which is known as the “City of Good Neighbors.” In Luke 10, Jesus was asked, “And who is my neighbor?” (Luke 10:29b). Our Lord answered by sharing the well-known story of the Good Samaritan. I believe with all my heart that God loves my hometown of Buffalo, as He does every city in our nation. He has great plans for healing our land (2 Chronicles 7:14).
As Buffalonians, from generation to generation, we have consistently demonstrated that we truly care about each other and are willing to generously help struggling, hurting people turn their lives around. The Lord is calling all of us to be Good Samaritans as Jesus taught, and I believe the church is the safe inn for hurting people to heal. We believe the abundant life spoken of in John 10:10 is living in communion with God and community with each other. For all of our sons and daughters who are far from home, the parable of the prodigal son inspires us to never give up hope. Luke 15:20 shares the story of a son who was still a long way off when his father saw him coming. Filled with love and compassion, the father ran to his son and EMBRACED him.
Embrace Recovery Buffalo
Embrace Recovery Buffalo was birthed in 2016 out of a desperate heart cry and a mission to help those struggling with addiction or life-controlling problems find compassion, hope, healing and lifelong recovery through a collaborative effort that includes a biblical faith-based approach. Just like the father embraced his lost son, we seek to embrace those who are lost and searching through the fog of addiction.
Western New York is home to the nationally recognized Erie County Opiate Epidemic Task Force, whose efforts are making significant strides with a collaborative approach that is producing results. The task force has strong relationships with law enforcement and the nation’s first opioid intervention court. In addition, the University at Buffalo (UB) is fighting addiction through research education and clinical care. UB has more than 150 faculty and scientists (including fellow CMDA members) investigating addiction, and they are educating students in all of the health science disciplines (medicine, nursing, social work, pharmacy, dentistry and public health).
UB’s Clinical and Research Institute on Addictions (CRIA) is a long-standing leader in the study of alcohol and substance use disorder. Dr. Richard Blondell, who is a national leader in addiction medicine, developed an addiction medicine fellowship in UB’s Department of Family Medicine in 2011. It is one of the nation’s first post graduate addition medicine fellowships. For many years, UB’s Faith and Medicine elective has provided medical students opportunities to see how a life filled with faith can powerfully impact the lives of our patients. The elective allows medical students to visit many Embrace Recovery Buffalo Community Connections and hear powerful testimonies that will be remembered for a lifetime.
Our Community Connections include: Adult and Teen Challenge, founded by Pastor David Wilkerson with more than 220 residential program locations across North America; Total Freedom Darien, which has a faith-based residential rural campus; Kids Escaping Drugs, that helps to educate in addition to treatment; and Buffalo City Mission. Healthcare students also have academic opportunities at large organizations that have been dedicated to addiction and mental healthcare in Western New York for decades.
“My journey has been a very long one, including not a denial that there is a Lord but more of a ‘I don’t need Him.’ At the darkest time in my life, the Holy Spirit visited with an incredibly strong message of hope. Since then, I have searched and found help with physicians who have encouraged me and provided assistance with pharmaceutical interventions. The road was still quite bumpy, but eventually with faith, hope and a lot of love I found a way forward. There is a tremendous network of believers out there who can give you hope and a way to grace if you’re open to it. Pass it on.”
—Doug
Caring for those suffering with addiction and commonly co-occurring mental health conditions, such as anxiety and depression, is a vitally important local mission to our community and our team. Having mercy on those with conditions of despair, we become the hands and feet of Jesus in our city as we seek to rescue, recover and restore.
Our team continues to educate, equip and engage healthcare professionals, patients and families in our community to shed light on the stigma and ignorance that shroud addiction. Addiction care is just as important as any other type of healthcare. Similar to other chronic health conditions such as diabetes, heart disease and cancer, substance and alcohol use disorder can be successfully screened, diagnosed and effectively treated in primary care, hospital, emergency room, behavioral health and other clinical settings. We train healthcare professionals to use tools such as Screening Brief Intervention and Referral to Treatment (SBIRT) and motivational interviewing.
Hub and Spoke—The Importance of Partnerships
I believe the key to success in making a difference in our community’s struggle with opioids is found in building and strengthening relationships and partnerships. That includes implementing both clinical and community care teams in a growing regional “hub and spoke” model of care that was launched from a UB Addiction Medicine Fellowship Project. Treatment plans of care include evidence-based effective medications, mental health counseling, recovery coaching and thriving community support groups.
In Buffalo, we have trained several dozen life recovery coaches in churches, ministries and organizations that are an integral part of the community care team that leads people on their path to recovery in a variety of clinical and community settings. Recovery coaches guide and support people to achieve and maintain the goals of recovery. Our vision is to educate, equip and engage coaches in every church, and in each neighborhood, to create a safety net, understanding God’s heart that none shall perish. It says in 2 Peter 3:9, “The Lord is not slow about His promise, as some count slowness, but is patient toward you, not willing for any to perish, but for all to come to repentance” (NASB).
To help accomplish that vision, we provide free recovery Bibles, journals, biblical resources and educational tools to equip healthcare professionals, students, organizations, ministries, patients and families.
“When I envisioned my role as a recovery coach, I see two people walking shoulder to shoulder, one, the recoveree, working the self-selected process toward recovery. The coach, supporting by promoting recovery with community support services as useful, encouraging hope, positivity, health and a personal relationship with God.”
A Time to Embrace
The addiction crisis continues to claim tens of thousands of lives each year. Sadly, current evidence suggests worsening of disparities in access to care and mortality of the underserved. The need to identify and treat has never been more urgent. Out of 10 people who suffer from substance use disorder or alcohol use disorder, only one or two receive appropriate care. Only one or two…out of 10. It’s a disheartening and eye-opening statistic. Hurting people deserve the same compassionate care we all expect from our healthcare professionals, and that means we need to work together to treat people with love, dignity and respect. Addiction medicine is our opportunity to collaborate together as we teach “medicine to ministry” and “ministry to medicine.”
The Bible story found in the gospels of Matthew, Mark and Luke describe the four faithful friends carrying a paralytic. That gospel story also tells our Embrace Recovery Buffalo story.
The four faithful friends were purpose driven, dedicated and intentional, and they demonstrated perseverance with sacrificial love by punching a hole in the roof to bring a lame hurting friend to Jesus, the Great Physician. Our Lord Jesus embraced the hurting and broken. The faithfulness of the four friends resulted in the awesome healing of spirit, soul and body! As it says in Psalm 133:1, “How good and pleasant it is when God’s people live together in unity!”
Each friend did their part to complete the mission. Ephesians 4:12 says, “to equip his people for works of service, so that the body of Christ may be built up.”
At Embrace Recovery Buffalo, our prayer is that we may all have the courage and strength to do the same. Which friend are you? Are you the educator, healthcare professional, student, law enforcer, recovery coach, loved one, counselor, neighbor, teacher, researcher, athlete, etc.? The Lord is equipping you with the tools, the networks and the connections you need to follow His will and to allow Him to work through you. Are you ready to embrace recovery?
About the Author
Darren Caparaso, MD, is a family medicine and addiction medicine physician. He is the Founder and Co-director of Embrace Recovery Buffalo, a ministry affiliated with CMDA with the mission to help those struggling with addiction or life-controlling problems find compassion, hope, healing and lifelong recovery through a collaborative effort that includes a biblical faith-based approach. He serves as the Addiction Medicine Section Outreach Coordinator. For more information about Embrace Recovery Buffalo, visit www.cmdawny.org/embrace-recovery-about.
Get Involved
The Addiction Medicine Section of CMDA exists to prevent and treat addiction and transform lives, by God’s grace, love and power. We strive to provide compassionate excellence in all aspects of addiction care, including whole-person prevention and treatment, education, advocacy, empowerment of others, research, church, and community partnerships, and interprofessional collaboration and support. For more information and to get involved, visit www.cmda.org/ams.
SECOND PIECE
Building a Foundation to Recovery
by David Holmes, MD
Numerous medical research studies support the idea that health and well-being are affected by four main aspects of a person’s life: physical, psychological, social and spiritual. These aspects also affect recovery from addictions to drugs, alcohol, tobacco, sex, gambling, etc. This is called the bio-psycho-social-spiritual model of whole-person healthcare. I use this model when taking a patient’s history and recommending a treatment plan. So much of healthcare is focused on the biological or physical aspects of health. We need to learn and strive to provide excellent physical medical care. However, I think all healthcare professionals should also strive to provide excellent psycho-social-spiritual medical care.
When asking psycho-social-spiritual questions, I often ask patients about their biggest stressors and how they cope with them. Probably half of the inpatients I see on a general medical floor in a local hospital are there because of unhealthy ways of coping with stress, anxiety, sadness, boredom or loneliness. These unhealthy coping strategies, such as smoking, overeating, alcohol, inactivity, anger, drugs, isolation, inactivity, etc., can contribute to problems including ulcers, cirrhosis, heart disease, seizures, injuries, anxiety, some types of cancer, etc. This doesn’t mean these problems are always, or even usually, caused by unhealthy coping strategies, as other factors contribute to these conditions. However, for a number of people, unhealthy coping strategies likely contribute to their health problems.
Once I identify a patient has unhealthy coping strategies, I work with them to identify healthy coping strategies they could use instead. Some of these strategies include exercising, praying, listening to peaceful music, going for a walk, reading Scripture, journaling, doing a hobby they enjoy and talking with someone they trust, like a friend, family member, pastor or counselor. I also use the bio-psycho-social-spiritual model when I’m working with the patient to formulate a treatment plan. We focus on items they think they can start doing, and then I document the action points in the electronic health record so I can remember to follow up with them at future visits.
A number of years ago, I heard Dr. John Patrick talk about the four levels of happiness on CMDA’s Christian Doctor’s Digest (now called CMDA Matters). Ever since, I’ve included that material in required seminars I teach to medical students about whole-person healthcare. I also use this material in talking with patients who are struggling with addictions.
- Animal Happiness (short-term, self-focused)
You may be unhappy or grumpy because you’re hungry. Then you eat a big meal and you’re happy. A few hours later, you can repeat the whole process again. The same is true if you’re tired and then get some sleep. Other examples of short-term happiness include sex, shelter, health, things, money, pornography, smoking, drugs, alcohol, shopping, etc. Some of these things do bring happiness, but it’s on a short-term basis. Some things can lead to unhappiness. For instance, too much eating can lead to obesity. Smoking and excessive alcohol use can lead to addictions and health problems.
- Accomplishments (self-focused)
Accomplishments provide a deeper sense of happiness and satisfaction. Some examples include doing well on an exam, receiving an award, accomplishing chores at home, getting a good job, reaching a goal, winning a competition, etc. These provide a little deeper sense of happiness and satisfaction in life. However, there are lots of people with great jobs who are still miserable. Therefore, we need more than just our accomplishments to be happy and content.
- Relationships and Service (others-focused)
Unlike the previous two levels, this level focuses on others. Some examples include relationships with your spouse, children, relatives, friends, co-workers, patients and others. It’s also about serving others, such as volunteering and giving of your time, talents and treasure. We all have a need to be needed, so helping others also helps ourselves. However, relationships sometimes don’t work out well. Sometimes, marriages end in divorce. Children grow up and leave the home. Some children rebel. There may be conflicts and tension with friends. Loved ones may die. Then what do we do? We need to rely on our foundation.
- Foundation (God-focused or beliefs-focused)
Examples of a foundation are faith, beliefs, values, culture, identity and integrity. The first three levels of happiness can all be taken away from you. Your foundation is the part of you that can never be taken away. It gives you meaning and purpose in life and can help you through the storms and challenges of life.
The purpose of the foundation of a building is to help it stay standing when storms and bad weather hit. Without a strong foundation, the building may crack and collapse. The same is true with our lives. If we have a weak foundation, then, when the storms and problems hit, we will struggle with those things, because they are difficult. However, if we have a strong foundation, we’ll be able to stay standing and move forward with our lives. If we don’t have a strong foundation, then when the storms arrive, we’re going to collapse. There will be problem on top of problem, and it will be difficult to dig our way out. When I get to this point with patients, they often relate to having a collapsed life with problems piling on top of one another. At this point, even patients who don’t profess much in terms of spiritual beliefs begin to understand the importance of having a strong foundation. This can open the door to a conversation about how faith can help in building a strong foundation.
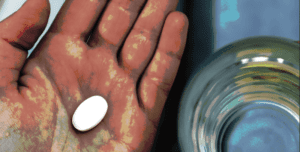
If I sense a patient might be interested, I’ll offer them a Life Recovery Bible, which is donated by Embrace Recovery Buffalo. This Bible is filled with explanations about how certain passages in the Bible relate to the 12 steps of Alcoholics Anonymous or Narcotics Anonymous. I suggest they read a few verses each day. Just as having physical food each day helps nourish our bodies, having spiritual and inspirational food each day helps nourish our souls and strengthen our foundation. Some patients like to journal or are open to doing it. I often offer these patients the Recovery Journal, which is also provided free of charge by Embrace Recovery. Each day has a Scripture verse and brief devotional, followed by space for them to journal a response. If I don’t sense they would be interested in either the Bible or the journal, I offer The Daily Bread devotional booklet, which is available in bulk at no cost from odb.org/getprint. I try to offer it in a non-pushing way, so they don’t feel obligated to take one.
In terms of praying with patients, here are the general guidelines I use:
- I usually only ask patients if they would like prayer if I’m almost certain they will say yes. Taking a spiritual history usually helps me to know if a patient will appreciate prayer or not.
- Some people believe it is best to only pray with a patient if the patient initiates a request for it. That may be the best indication for praying with a patient, but the problem is that it is not common for healthcare professionals to pray with patients. Therefore, most patients wouldn’t even think to ask you to pray for them, especially if they don’t know if you do that with patients. Therefore, it’s up to Christian healthcare professionals to somehow communicate this to their patients. I choose to do that by asking, in a nonjudgmental way, if they would like me to pray for them.
- If the patient says they would like prayer, then I ask them what prayer requests they have. This helps me to know what to focus my prayer on, and it also gives me a glimpse into what’s going on in their heart.
- In general, my prayers are brief and focused on the patient’s prayer requests. I also include gratitude for something positive going on in the patient’s life and/or aspects of God’s character, such as His love and help that He freely gives us. Finally, I often include parts of the treatment plan, such as for God to help them quit smoking.
- I document prayers in the medical record; that way, when I see the patient again, I can be reminded of the fact that we prayed and what we prayed for. If I don’t document this and I don’t remember, then when I see the patient and don’t ask about how things are going with whatever we prayed for, it may appear that I am uncaring about what the patient was struggling with during the previous visit.
I work in a county hospital and clinic, plus I’m on faculty at a state medical school. In 27 years of medical practice and addressing spiritual issues with patients, I’ve had countless positive and meaningful moments with patients, as addressing these issues often strengthens trust and rapport. In that time, I’ve only received a couple complaints from administrators about my faith-based approach to patient care. I simply explain the truth—that I’m practicing evidence-based, patient-centered, whole-person healthcare. There’s not much they can say in response to that. At the end of my conversation with one of the administrators, she asked if she could have one of the Life Recovery Bibles that I give to patients and if I’d be willing to teach the clinic staff about spirituality in health. Of course, I said yes to both. It’s amazing how God can use all sorts of things to share the truth of His Word and the valuable role faith plays in our health and well-being, especially when it comes to creating a strong foundation in recovery from addiction.
About the Author
David Holmes, MD, is a Clinical Associate Professor in the Department of Family Medicine, Jacobs School of Medicine and Biomedical Sciences, SUNY at Buffalo (UB). He is board certified in family medicine and addiction medicine. He directs the Global Medicine Program and the spirituality in medicine curriculum for the medical school. He’s an Associate Program Director for the family medicine residency program. His research interests focus on global health and the role of faith in addiction recovery. He says that his personal mission statement is “to love and honor God and my family and make a positive and significant difference in the lives of others.”